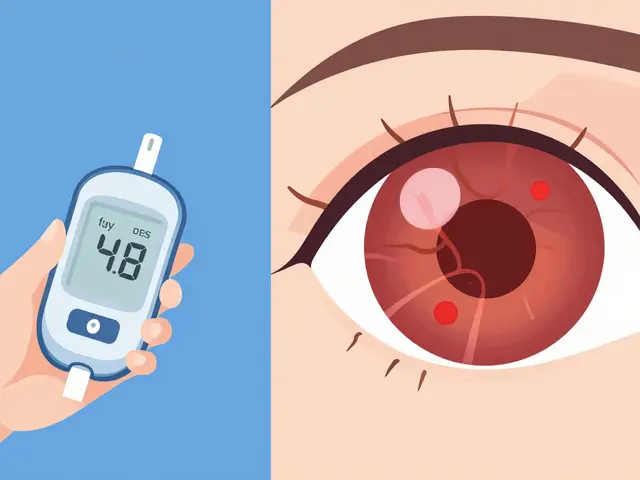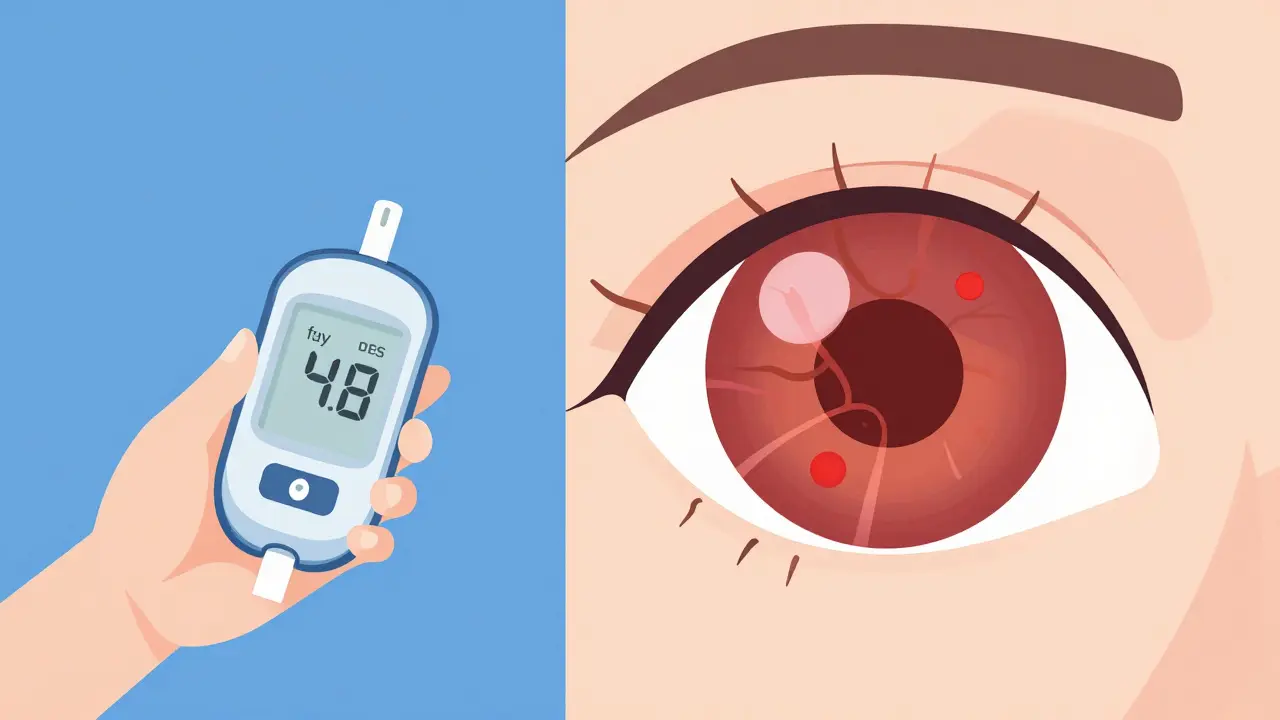
Most people with diabetes think about their blood sugar numbers first. They check glucose levels, adjust insulin, and watch what they eat. But there is a silent threat that doesn't show up on a glucometer: damage to the eyes. Diabetic retinopathy is the leading cause of vision loss in working-age adults, yet it often has no early symptoms. You can have perfect 20/20 vision while your retina is deteriorating. This is why diabetic eye screening isn't just a recommendation-it's a critical part of survival.
The good news? More than 90% of diabetes-related vision loss is preventable if caught early. The bad news? Only about 60% of people with diabetes actually get their recommended annual exams. Why the gap? Transportation issues, fear of dilation drops, and long wait times for specialists play a huge role. That’s where new technology steps in. Teleophthalmology and AI-driven diagnostics are changing how we catch these problems before they become permanent.
Who Needs an Eye Exam and When?
You might assume you only need an eye doctor if your vision gets blurry. That’s a dangerous myth. Diabetes damages the tiny blood vessels in the retina long before you notice any change in how things look. The timing of your first exam depends entirely on which type of diabetes you have.
If you have Type 1 diabetes, a chronic condition characterized by high blood sugar levels resulting from the pancreas' inability to produce insulin, your body has been fighting high glucose since diagnosis. However, retinopathy takes time to develop. The American Diabetes Association (ADA) 2025 Standards of Care recommend your first comprehensive dilated eye exam within five years after your initial diagnosis. If you were diagnosed as a child, this timeline starts from when you were first identified as having the disease.
For those with Type 2 diabetes, a metabolic disorder marked by insulin resistance and relative insulin deficiency, the rules are stricter. High blood sugar may have been damaging your eyes for years before you even knew you had diabetes. Therefore, you need a dilated eye exam at the time of diagnosis. Do not wait. Do not assume your last optometrist visit counts-that was likely a refraction test for glasses, not a medical evaluation of the retina.
How Often Should You Get Screened?
Once you start screening, the frequency depends on what the doctor sees. It’s not a one-size-fits-all schedule. Here is how the intervals break down based on current clinical guidelines:
- No Retinopathy Found: If your eyes are healthy and your blood sugar is well-controlled (HbA1c below 7%), you typically need an exam every year. Some recent studies suggest that for very low-risk patients, extending this to every two years might be safe, but annual checks remain the gold standard.
- Mild Nonproliferative Diabetic Retinopathy (NPDR): If early signs appear, such as microaneurysms, you’ll likely need follow-ups every 6 to 12 months. The goal here is to stop progression.
- Moderate to Severe NPDR: As damage worsens, the risk of bleeding or fluid leakage increases. Exams shift to every 3 to 6 months. In severe cases, monthly checks may be required.
- Proliferative Diabetic Retinopathy or Macular Edema: These are advanced stages. Proliferative DR involves abnormal blood vessel growth, while macular edema is swelling in the central part of the retina. Both require treatment and monitoring every 1 to 4 months, depending on response to therapy.
Dr. Ildiko Lingvay, Chair of the ADA 2025 Standards Committee, emphasizes that skipping exams drastically increases risk. Data from the Wisconsin Epidemiologic Study shows a 23-fold increase in vision loss for patients who miss recommended screenings. Consistency matters more than perfection in blood sugar control when it comes to preserving sight.
What Happens During a Traditional Screening?
A standard diabetic eye exam is more thorough than a routine vision check. It usually involves three key steps:
- Dilation: The doctor puts drops in your eyes to widen the pupils. This lets them see the entire retina, including the peripheral areas where damage often starts first. The downside? Your vision will be blurry and sensitive to light for several hours. Many patients cite this discomfort as a reason to delay appointments.
- Fundus Examination: Using a special lens, the ophthalmologist or optometrist looks for hemorrhages, exudates (leaked fluid), and neovascularization (new, fragile blood vessels).
- OCT Imaging: Optical Coherence Tomography creates cross-sectional images of the retina. This is crucial for detecting diabetic macular edema, which can’t always be seen with the naked eye.
While effective, this process requires travel to a specialist, time off work, and dealing with post-dilation inconvenience. For millions of people, especially those in rural areas, these barriers lead to missed care.
Enter Teleophthalmology: A Game Changer
Teleophthalmology allows eye care professionals to diagnose retinal diseases remotely. Instead of traveling to a clinic, you go to a primary care office, community center, or even a mobile unit equipped with a specialized camera. They take high-resolution photos of your retina without needing dilation in many cases. These images are then sent to a grader-a trained technician or ophthalmologist-who reviews them for signs of disease.
This model has proven highly effective. In a large-scale project in Tamil Nadu, India, remote graders agreed with in-person specialists in 98.5% of cases across 15,000 screenings. Closer to home, the Veterans Health Administration saw a 32% jump in screening completion rates after rolling out teleophthalmology across 136 facilities. Why? Because it removes the friction. You don’t need to drive 75 miles to see a specialist. You don’t need to worry about driving home with blurred vision.
But does it replace the doctor? Not entirely. Retinal photos are excellent for spotting diabetic retinopathy, but they don’t detect other eye issues like glaucoma or cataracts. Think of teleophthalmology as a powerful filter. It catches the urgent diabetic complications quickly. If something looks suspicious, you’re referred for a full in-person exam. If everything looks clear, you stay on track with your next scheduled screen.
AI and FDA-Approved Diagnostics
The latest twist in this story is artificial intelligence. Systems like IDx-DR (now LumineticsCore) use algorithms to analyze retinal images automatically. Approved by the FDA in 2018, this system can detect referable diabetic retinopathy and macular edema with 87.2% sensitivity and 90.7% specificity. That means it correctly identifies most serious cases while minimizing false alarms.
In 2025, the ADA officially endorsed AI-assisted screening as a valid alternative to traditional methods, provided the system meets regulatory standards. Currently, FDA-cleared AI systems cover about 22% of Medicare diabetes screenings, up from just 8% in 2022. This rapid adoption makes sense. Primary care doctors can run the scan during a regular checkup. The patient gets immediate results. No referral lag. No lost paperwork.
However, access remains uneven. A 2024 Health Affairs study found that clinics serving predominantly Medicaid patients adopted teleophthalmology at rates 47% lower than those serving commercially insured patients. We’re solving a logistical problem but potentially widening an equity gap. Ensuring all patients benefit from these tools is the next challenge.
| Feature | Traditional In-Person Exam | Teleophthalmology | AI-Assisted Screening |
|---|---|---|---|
| Scope | Comprehensive (retina, glaucoma, cataracts) | Retina-focused (DR/DME detection) | Retina-focused (automated DR/DME detection) |
| Dilation Required? | Yes, almost always | Sometimes (depends on camera quality) | Rarely (non-mydriatic cameras used) |
| Time Commitment | 1-2 hours (including recovery) | 15-30 minutes | 10-15 minutes |
| Accessibility | Low in rural areas | High (can be done in primary care) | Very High (point-of-care) |
| Best For | Initial diagnosis, complex cases | Regular monitoring, underserved populations | High-volume screening, quick triage |
Barriers to Getting Screened-and How to Overcome Them
Even with better technology, people still skip exams. Understanding why helps us fix it.
Transportation is the biggest hurdle. A 2023 survey by the National Federation of the Blind found that 68% of patients cited travel difficulties as the main reason for missing appointments. If you live in a rural area, ask your primary care provider if they offer on-site teleophthalmology. Many community health centers now have retinal cameras. If not, look into local transportation assistance programs offered by Area Agencies on Aging or disability services.
Fear of dilation is real. About 42% of patients report discomfort from pupil dilation as a deterrent. Remember, non-dilated imaging is becoming common in teleophthalmology setups. Ask your provider if they use non-mydriatic cameras. While dilation gives the clearest view, modern wide-field cameras often provide sufficient detail for screening purposes.
Misinformation spreads easily. A 2024 University of Michigan study revealed that 58% of patients wrongly believed that normal blood sugar alone prevents all eye complications. It doesn’t. Genetics, duration of diabetes, blood pressure, and cholesterol also play roles. Even with perfect HbA1c, you need screening. Talk to your endocrinologist about your individual risk profile.
Insurance confusion adds stress. While Medicare covers preventive eye exams for diabetics, coverage for teleophthalmology varies. As of 2024, only 63% of private insurers covered remote eye screenings. Check your plan details. If it’s not covered, ask if the service can be billed under primary care visits or chronic disease management codes.
Practical Steps to Stay on Track
Don’t leave your eye health to chance. Here’s a simple action plan:
- Know your baseline. If you’ve never had a dilated exam, schedule one immediately. Note the date and results in your health records.
- Set recurring reminders. Use your phone calendar or ask your clinic to send SMS alerts. Kaiser Permanente reduced missed appointments by 27% using automated texts sent 21, 14, and 7 days before exams.
- Coordinate with your team. Share your eye exam results with your primary care doctor and endocrinologist. They need to know if your retinopathy is progressing, as it may signal poor systemic control.
- Explore local options. Search for "teleophthalmology near me" or ask your pharmacy if they host screening events. Some retail vision chains now partner with telehealth providers.
- Advocate for yourself. If you’re told you “don’t need an exam” because your vision is fine, push back. Cite the ADA guidelines. Insist on a referral if necessary.
Looking Ahead: Personalized Screening Intervals
The future of diabetic eye care isn’t just about better cameras-it’s about smarter scheduling. Researchers at the T1D Exchange are developing algorithms that consider 17 risk factors beyond HbA1c, including age, race, blood pressure variability, and lipid profiles. The goal? To safely extend screening intervals to every three years for truly low-risk patients, freeing up resources for those who need frequent monitoring.
However, experts warn against over-extending intervals too soon. Dr. Michael F. Chiang of the National Eye Institute notes that minority populations often experience faster retinopathy progression despite similar glycemic control. African American patients, for instance, develop proliferative retinopathy 2.3 years earlier than Caucasian patients with identical HbA1c levels. One-size-fits-all extensions could disproportionately harm vulnerable groups. Equity must guide innovation.
Can I skip my eye exam if my blood sugar is well-controlled?
No. While good blood sugar control significantly reduces risk, it does not eliminate it. Other factors like high blood pressure, cholesterol, and genetics contribute to retinopathy. The ADA recommends annual exams regardless of HbA1c levels unless specific low-risk criteria are met and approved by your doctor.
Is teleophthalmology as accurate as seeing an eye doctor in person?
For detecting diabetic retinopathy and macular edema, yes-studies show agreement rates above 98% between remote graders and specialists. However, teleophthalmology focuses primarily on the retina. It may miss other conditions like glaucoma or cataracts, so periodic comprehensive in-person exams are still important.
Do I need dilation for a diabetic eye screening?
Traditionally, yes. Dilation allows the doctor to see the entire retina clearly. However, many teleophthalmology programs use non-mydriatic (non-dilated) cameras that capture sufficient detail for screening purposes. Ask your provider which method they use and whether dilation is necessary for your case.
How much does a diabetic eye exam cost?
Medicare Part B covers preventive diabetic eye exams once per year for eligible beneficiaries with little to no out-of-pocket cost. Private insurance coverage varies; some plans cover it fully, while others may charge a copay. Teleophthalmology services may have different billing codes, so verify coverage with your insurer beforehand.
What should I do if I find out I have diabetic retinopathy?
Don’t panic. Early-stage retinopathy often doesn’t require immediate treatment but needs closer monitoring. Work with your eye doctor to establish a follow-up schedule. Tighten control of your blood sugar, blood pressure, and cholesterol. Treatments like laser therapy, injections, or surgery are available for advanced stages and can preserve vision effectively.