
Empagliflozin vs Alternatives: Drug Selector
Select Your Priorities
Recommended Medication
Quick Takeaways
- Empagliflozin is an SGLT2 inhibitor that lowers blood sugar and reduces heart‑failure risk.
- Canagliflozin, dapagliflozin and ertugliflozin share the same class but differ in kidney safety and dosing.
- Metformin remains the first‑line oral drug; it works via a completely different pathway.
- GLP‑1 agonists like semaglutide excel at weight loss and cardiovascular protection but require injections.
- Choosing the right drug depends on heart health, kidney function, weight goals and tolerance for side‑effects.
When you’re sorting through diabetes meds, the choices can feel overwhelming. Empagliflozin often pops up because it’s praised for heart‑failure benefits, but how does it really stack up against the other options on the market? This guide walks you through the science, the numbers, and the practical trade‑offs so you can decide which pill (or injection) fits your health goals.
What is Empagliflozin?
Empagliflozin is a prescription medication that belongs to the sodium‑glucose co‑transporter‑2 (SGLT2) inhibitor class. It works by blocking glucose reabsorption in the kidneys, causing excess sugar to be expelled in urine. Approved by the FDA in 2014, it quickly became a favorite for patients with type 2 diabetes who also have cardiovascular risk.
How Empagliflozin Works
The kidneys filter about 180 grams of glucose each day. Under normal conditions, SGLT2 proteins grab most of that sugar and send it back into the bloodstream. Empagliflozin plugs that plug‑hole, so roughly 60‑80 grams of glucose leave the body every day. The result is lower blood‑sugar levels, modest calorie loss, and a dip in blood pressure.
Key Benefits of Empagliflozin
- Reduces HbA1c by 0.7‑1.1% on average.
- Triggers 2‑3kg of weight loss over 6months.
- Cut risk of major adverse cardiovascular events (MACE) by 14% in the EMPA‑REG OUTCOME trial.
- Lowers hospitalization for heart failure by 35%.
- Offers some kidney‑protective effects, slowing eGFR decline.
Who Typically Takes Empagliflozin?
It’s prescribed for adults with type 2 diabetes, especially those who have established cardiovascular disease or are at high risk for heart failure. Doctors also consider it for patients with mild‑to‑moderate chronic kidney disease (CKD) because the drug works even when kidney function drops to an eGFR of 30mL/min/1.73m².
Alternative SGLT2 Inhibitors
While Empagliflozin often steals the spotlight, other SGLT2 inhibitors are widely used. Below are quick snapshots of the most common ones.
Canagliflozin debuted a year before Empagliflozin and is marketed under the brand name Invokana. It shares the same glucose‑excretion mechanism but has a slightly higher risk of lower‑leg amputations, which led to a black‑box warning in 2017.
Dapagliflozin, sold as Farxiga, gained attention for its strong evidence in slowing CKD progression. It’s also approved for reducing heart‑failure hospitalization in patients with preserved ejection fraction.
Ertugliflozin (Steglatro) entered the market later and is often paired with metformin. Its dosing flexibility (5mg or 15mg) makes it a good option for people who need a gentle start.
Non‑SGLT2 Alternatives
For patients who can’t tolerate SGLT2 blockers-or whose doctors want a different approach-there are a few solid options.
Metformin remains the first‑line therapy for type 2 diabetes worldwide. It lowers hepatic glucose production and improves insulin sensitivity, typically reducing HbA1c by 1‑2% without causing weight gain.
Semaglutide is a GLP‑1 receptor agonist administered as a weekly injection. It delivers up to 15% weight loss and cuts MACE risk by about 20% in the SUSTAIN‑6 trial, but the injection route can be a barrier for some.
Traditional Insulin therapy is reserved for later stages or when oral agents fail to achieve targets. It provides the most potent glucose‑lowering effect but carries hypoglycemia risk and requires careful dose titration.
Head‑to‑Head Comparison
| Drug | Mechanism | Key FDA Indications | Cardiovascular Benefit | Weight Change | Common Side Effects | Typical Dose |
|---|---|---|---|---|---|---|
| Empagliflozin | SGLT2 inhibition | Type 2 diabetes, heart‑failure, CKD | ↓ MACE 14%; ↓ HF hospitalization 35% | ‑2-3kg | UTI, genital infection, volume depletion | 10mg once daily (max 25mg) |
| Canagliflozin | SGLT2 inhibition | Type 2 diabetes, CKD, HF | ↓ MACE 11%; ↑ amputation risk | ‑2kg | UTI, genital infection, amputations | 100mg once daily (max 300mg) |
| Dapagliflozin | SGLT2 inhibition | Type 2 diabetes, CKD, HFpEF | ↓ CKD progression, ↓ HF hospitalization | ‑1.5kg | UTI, genital infection, hypotension | 10mg once daily (max 25mg) |
| Metformin | Reduced hepatic gluconeogenesis | First‑line Type 2 diabetes | Neutral or modest ↓ CV risk | Weight neutral | GI upset, lactic acidosis (rare) | 500mg-2g daily split |
| Semaglutide | GLP‑1 receptor agonist | Type 2 diabetes, obesity | ↓ MACE 20% (SUSTAIN‑6) | ‑10-15kg | Nausea, vomiting, pancreatitis (rare) | 0.5mg weekly (titrated to 1mg) |
Pros and Cons of Empagliflozin
Pros
- Strong evidence for heart‑failure and CV death reduction.
- Works even when kidney function is reduced.
- Simple once‑daily oral dose.
- Promotes modest weight loss without hypoglycemia (when used alone).
Cons
- Genital mycotic infections are more common, especially in women.
- Can cause dehydration or low blood pressure.
- Not suitable for type 1 diabetes due to ketoacidosis risk.
- Cost may be higher than generic metformin.
How to Choose the Right Medication
Think of drug selection like matching a shoe to a foot. You look at three main dimensions: heart health, kidney health, and personal preferences (weight goals, injection aversion, cost).
- Prioritize heart health? If you’ve had a heart attack or have heart‑failure, Empagliflozin or Dapagliflozin are top picks because of their proven CV benefits.
- Kidney disease? Dapagliflozin shows the strongest data for slowing CKD progression, but Empagliflozin is also safe down to eGFR30.
- Weight loss focus? GLP‑1 agonists like Semaglutide win big on the scale, but they require injections.
- Budget constraints? Metformin is the cheapest and still highly effective when paired with lifestyle changes.
- Side‑effect tolerance? If you’re prone to urinary infections, consider Metformin or a lower dose of an SGLT2 inhibitor.
Discuss these factors with your healthcare provider. They’ll look at your eGFR, HbA1c, and any cardiovascular history before writing a prescription.
Frequently Asked Questions
Can I take Empagliflozin with Metformin?
Yes. Most doctors start patients on Metformin and add Empagliflozin if blood‑sugar control needs an extra push or if there’s a cardiovascular benefit to capture.
Do SGLT2 inhibitors cause ketoacidosis?
Euglycemic diabetic ketoacidosis is a rare but real risk, especially in type 1 diabetes or during severe illness. That’s why SGLT2 inhibitors are labeled for type 2 diabetes only.
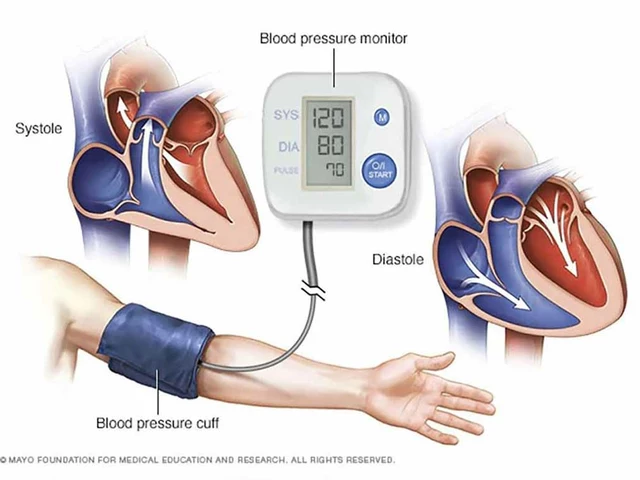
How fast does Empagliflozin lower blood pressure?
Most patients see a 3‑5mmHg drop in systolic pressure within a few weeks, thanks to its mild diuretic effect.
Is there a difference in cost between Empagliflozin and generic Metformin?
Metformin is available as a cheap generic, often under $10 per month. Empagliflozin is brand‑only in most markets and can cost $200‑$300 a month unless covered by insurance or a patient‑assistance program.
Can I switch from Canagliflozin to Empagliflozin?
Switching is usually straightforward: stop the old drug and start Empagliflozin the same day, unless you’ve had a recent infection or low blood pressure. Always confirm with your doctor.
Next Steps
If you’re already on an SGLT2 inhibitor, ask your clinician whether Empagliflozin’s cardiovascular data matches your health profile. If you’re starting medication for the first time, weigh the pros and cons above and bring a short list of questions to your next appointment. The right choice can keep your blood sugar steady, protect your heart, and even help you shed a few pounds.






Adam O'Rourke October 11, 2025
Wow, because we definitely needed another deep dive into SGLT2 inhibitors 🙄
Mary-Pat Quilty October 16, 2025
Oh dear, another *grand* showdown of pills, as if our pharmacies needed a drama club!
Empagliflozin waltzes in with its heart‑loving moves while dapagliflozin tries to steal the spotlight with kidney‑guarding pirouettes.
But let’s not forget our good old metformin, the quiet librarian of glucose control, always there with a whisper of cheapness.
And then there’s semaglutide, the flamboyant diva demanding an injection and a princely sum for a cameo.
Honestly, picking a drug feels like choosing a partner at a rave – you just hope they won’t leave you dehydrated.
Patrick McGonigle October 21, 2025
For anyone considering Empagliflozin, note that its cardiovascular benefit has been demonstrated in the EMPA‑REG OUTCOME trial, reducing major adverse cardiac events by about 14 %.
Keisha Moss Buynitzky October 26, 2025
I appreciate the concise summary, Dr. McGonigle. It is indeed essential for patients to discuss their individual risk factors with a clinician before initiating therapy.
Shivam yadav October 31, 2025
From my experience, the gentle approach of dapagliflozin works well for folks with moderate kidney impairment, though cost can be a barrier.
pallabi banerjee November 5, 2025
Thanks for sharing, Shivam. If anyone is worried about urinary infections, starting with a lower dose and staying hydrated can help mitigate that risk.
Alex EL Shaar November 10, 2025
Alright, let’s tear this apart. Empagliflozin gets a shiny medal for heart‑failure reduction, but the side‑effect list reads like a horror novella – genital yeast infections, volume depletion, and the ever‑looming ketoacidosis threat for the ill‑informed.
The pricing is absurd, especially when a generic metformin can be bought for pennies.
Don't get me started on the marketing hype; it’s a textbook case of pharma PR masquerading as science.
Anna Frerker November 14, 2025
Well, that was a masterpiece of complaining. If you’re so angry, maybe just stick to water.
Julius Smith November 19, 2025
Yo, this whole drug talk is 🔥🔥! Got any cheap hacks? 😎
Brittaney Phelps November 24, 2025
Hey Julius, while emojis are fun, remember the best “hack” is a balanced diet and regular exercise – they work with any medication.
Kim Nguyệt Lệ November 29, 2025
The information presented is accurate, though it could benefit from clearer formatting and consistent terminology.
Rhonda Adams December 4, 2025
Great point! Keeping the language consistent helps readers compare options more easily. 😊
Macy-Lynn Lytsman Piernbaum December 9, 2025
Alright, let’s zoom out and think about why we’re even having this conversation. 🌍
First, medicine is a reflection of our collective priorities – heart health, kidney health, weight loss, and cost all battle for dominance.
Second, each drug is a compromise, a trade‑off between efficacy and side‑effects, like choosing between chocolate and vanilla – both have merits, but you’ll never get both without paying the price.
Third, the SGLT2 class, headed by Empagliflozin, introduced a paradigm shift: we’re no longer just lowering glucose, we’re protecting organs.
Fourth, the cardiovascular benefit of Empagliflozin, proven in EMPA‑REG, is not a fluke; it’s a reproducible reduction in MACE that has changed guidelines.
Fifth, dapagliflozin’s kidney‑protective data is compelling, especially for patients with eGFR < 45 ml/min, where Empagliflozin’s evidence is slightly less robust.
Sixth, the risk profile matters – genital infections are common, and the rare ketoacidosis looms like a dark cloud for type‑1 patients.
Seventh, cost cannot be ignored; a brand‑only drug can drain wallets faster than a credit card bill after a holiday sale.
Eighth, generic metformin remains the cost‑effective workhorse, offering modest glycemic control without the glamour of flashy headlines.
Ninth, semaglutide brings dramatic weight loss, but the injection requirement and price tag make it a niche choice for motivated patients.
Tenth, patient preference is king – a needle‑averse individual will likely gravitate toward oral agents, while the highly motivated weight‑loss seeker might accept injections.
Eleventh, real‑world adherence often deviates from trial perfection; convenience and tolerability drive long‑term success.
Twelfth, clinicians must individualize therapy, weighing comorbidities, life expectancy, and socioeconomic factors.
Thirteenth, the future may bring combination pills that merge SGLT2 inhibition with GLP‑1 agonism, simplifying regimens even further.
Fourteenth, education is vital – patients need clear, jargon‑free explanations of benefits and risks.
Finally, the best drug is the one a patient will actually take consistently, because efficacy without adherence is meaningless. 🚀
Alexandre Baril December 14, 2025
Excellent summary, Macy‑Lynn. In practice, I find that discussing both the clinical data and the patient’s daily routine leads to a shared decision that improves adherence.