
Opioid Risk Stratification Calculator
Patient Risk Assessment
This tool calculates your patient's risk level for opioid misuse using the Opioid Risk Tool (ORT) criteria. Results help determine appropriate urine drug testing frequency for safe opioid management.
How it works: Answer 5 questions about patient history. Scores determine risk level: Low (0-1), Moderate (2-3), or High (4-5).
Risk Assessment Results
When patients are prescribed opioids for chronic pain, doctors aren’t just trying to manage pain-they’re trying to keep them alive. Opioid misuse and overdose deaths remain a serious public health issue, with over 80,000 deaths in the U.S. in 2021 involving opioids alone. One of the most common tools doctors use to reduce risk is urine drug screening. But it’s not as simple as checking if someone took their pills. The real challenge is knowing what the results mean-and when to trust them.
Why Urine Drug Screens Are Used in Opioid Treatment
Urine drug screens aren’t about punishment. They’re about safety. The goal is to make sure patients are taking their prescribed medication as directed and not using other substances that could be deadly when mixed with opioids. Fentanyl, cocaine, benzodiazepines, and even some over-the-counter cold medicines can turn a safe dose into a fatal one. The Centers for Disease Control and Prevention (CDC) recommends urine testing for anyone on long-term opioid therapy. It’s not because doctors don’t trust patients-it’s because they need objective data. A patient might swear they’re only taking oxycodone, but their urine might show traces of heroin or fentanyl. That’s not a lie-it’s a sign the treatment plan needs to change. Urine testing also helps catch drug diversion. Some patients sell their pills. Others get prescriptions from multiple doctors. A negative test for a prescribed opioid, or a positive test for an unprescribed one, can trigger a conversation instead of an accusation.How Urine Drug Tests Work: Immunoassays vs. Confirmatory Tests
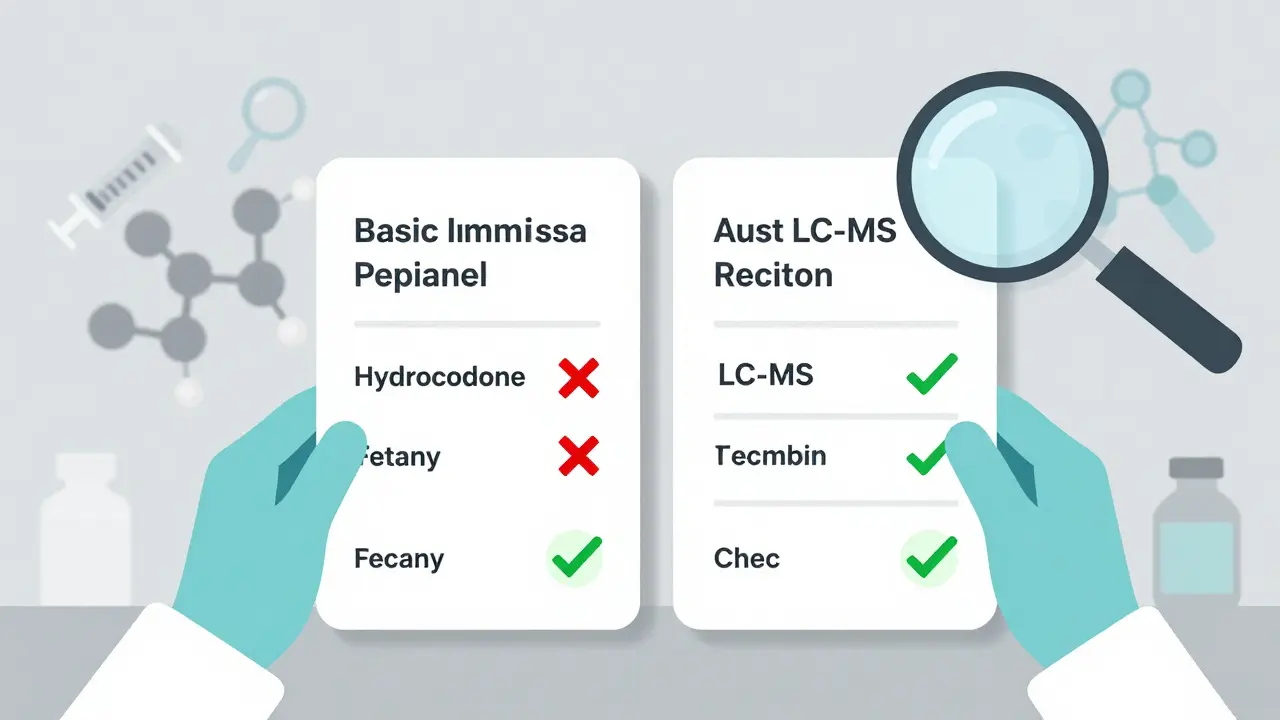
Not all urine tests are created equal. There are two main types: screening tests and confirmatory tests. Screening tests, usually immunoassays like EMIT, are cheap-around $5 per test-and give results in hours. They’re great for catching the big stuff: morphine, codeine, oxycodone, and methadone. But they have major flaws. Up to 30% of results can be false positives. Common medications like poppy seeds, ibuprofen, or even some antidepressants can trigger a positive for opioids. Worse, many standard screens miss hydrocodone entirely. One study found that 72% of patients who were taking hydrocodone tested negative on routine screens. That’s why confirmatory tests like GC/MS or LC-MS are critical. These lab-based methods identify exact drug molecules, not just broad categories. They cost more-$25 to $100 per test-but they’re accurate. If a screening test shows a positive for opioids, a confirmatory test tells you whether it’s oxycodone, heroin, or something else entirely. Fentanyl is a huge blind spot. Most standard immunoassays can’t detect it because its chemical structure is too different from morphine. Until 2023, doctors had no reliable way to know if a patient on a fentanyl patch was actually using it. Now, new FDA-approved fentanyl-specific immunoassays exist with 98.7% sensitivity. But many clinics still use outdated panels.What the Results Really Mean
A negative test for a prescribed opioid doesn’t always mean the patient isn’t taking it. It could mean:- The test doesn’t detect that specific drug (like hydrocodone on a standard opiate screen)
- The patient took the dose too recently or too long ago
- Their body metabolizes the drug differently
- The sample was diluted or substituted
- The patient is self-medicating for untreated anxiety or insomnia
- They’re using a friend’s medication after losing their prescription
- They’re unaware the drug is even in their system (like a contaminated supplement)
Risk Stratification: Who Needs Testing and How Often?
Not every patient on opioids needs quarterly urine tests. That’s where risk stratification comes in. The Opioid Risk Tool (ORT) is a simple 5-question survey that classifies patients as low, moderate, or high risk for misuse based on personal and family history of substance use, mental health conditions, and age. The American Medical Association now recommends testing frequency based on these categories:- Low risk: Annual screening
- Moderate risk: Every 6 months
- High risk: Every 3 months, plus specimen validity checks
Specimen Validity: Making Sure the Sample Is Real
A test result is only as good as the sample. That’s why labs check for validity before interpreting results. Three red flags:- Dilution: Specific gravity below 1.003-could mean the patient drank excessive water to flush the system
- Adulteration: Urine pH below 4.5 or above 9.0-suggests someone added bleach, vinegar, or commercial products to hide drugs
- Substitution: Creatinine below 20 mg/dL-could mean the sample came from someone else
Market Trends and Real-World Challenges
The urine drug testing market is booming-$3.1 billion in 2022 and growing. Thirty-eight U.S. states now require testing for patients on high-dose opioids. Medicare paid for nearly 39 million tests in 2022. But there’s a gap between policy and practice. A 2019 study found that 30% of urine tests ordered in pain clinics were clinically inappropriate. Some doctors test every patient every month, regardless of risk. Others still use outdated panels that miss fentanyl and hydrocodone. Major labs like Quest Diagnostics and LabCorp dominate the market, but their test panels vary. A patient might get a negative result at one clinic and a positive at another, simply because the lab used a different assay.What’s Next for Opioid Monitoring?
The future of opioid monitoring is smarter, not just more frequent. New tools are emerging:- Point-of-care devices: Handheld testers that give lab-quality results in minutes-seven are in FDA review as of late 2023.
- AI prediction models: The University of Pittsburgh’s Opioid Adherence Prediction Engine uses patient behavior, prescription refill patterns, and social factors to predict misuse risk before a test is even done.
- Updated guidelines: The CDC is expected to release new opioid monitoring guidelines in late 2024, emphasizing LC-MS for patients on synthetic opioids.
What Patients Should Know
If you’re on long-term opioid therapy:- Ask what drugs your urine test checks for-especially if you’re on hydrocodone or fentanyl.
- Bring a list of all medications, including supplements and OTC drugs.
- Don’t panic if your prescribed drug doesn’t show up. Ask if the test can detect it.
- Understand that a negative result doesn’t mean you’re being accused-it might mean the test has limits.
Do urine drug tests prove if someone is addicted to opioids?
No. Urine drug screens detect the presence of drugs in the system, not addiction. Addiction is a medical diagnosis based on behavioral, psychological, and physical criteria-not a positive or negative test result. A person can take opioids exactly as prescribed and still have an addiction. Conversely, someone who tests positive for an unprescribed drug may be using recreationally without meeting addiction criteria. Testing helps identify risk, not diagnose disorder.
Can I be punished for a positive drug test?
Legally, some clinics may terminate care after a positive test, but ethically, that’s not the right approach. The goal of testing is to identify risks and adjust treatment-not to punish. Many patients who test positive for unprescribed substances are self-medicating for untreated anxiety, trauma, or sleep issues. A better response is to explore underlying causes and offer support, not dismissal. The American Medical Association and CDC both recommend counseling and treatment adjustments over punitive actions.
Why do some prescribed opioids not show up in urine tests?
Many standard urine screens are designed to detect morphine-like opioids like codeine and oxycodone. Hydrocodone, hydromorphone, and fentanyl have different chemical structures and often don’t trigger these tests. Even if you take your full dose, the assay may miss it. This isn’t your fault-it’s a limitation of the test. Always ask your provider which specific drugs their lab screens for, and request confirmatory testing if a result seems inconsistent with your medication use.
Is it better to use blood instead of urine for opioid testing?
No. Blood tests show recent drug use-usually within hours-and are not practical for routine monitoring. Urine tests detect drug use over the past few days, which is more useful for tracking adherence. Blood tests are invasive, more expensive, and rarely needed unless there’s suspicion of acute overdose or impaired driving. Urine remains the standard for chronic opioid therapy monitoring because it’s noninvasive, cost-effective, and reflects longer-term patterns.
Can I refuse a urine drug test?
Yes, you can refuse. But if you’re on long-term opioid therapy, your provider may decide to stop prescribing opioids if you won’t participate in monitoring. This isn’t arbitrary-it’s a safety policy. Opioids carry serious risks, and without objective data, doctors can’t safely manage your care. Refusing testing doesn’t mean you’re guilty; it just means the risk is too high for the provider to continue prescribing without more information.






Kuldipsinh Rathod December 25, 2025
Man, this is so real. I’ve seen friends get shut down for a false positive on a test that didn’t even detect their actual med. No one’s trying to hide anything-they just want to feel seen, not judged.
Lori Anne Franklin December 26, 2025
they forgot to mention that some labs still use 10 year old panels 😭 i got tested last month and they missed my hydrocodone-i had to beg for a confirmatory test. why is this still a thing??
Ellie Stretshberry December 27, 2025
my doc switched to risk-based testing last year and it changed everything. i’m low risk, so i only get tested once a year. i actually feel trusted now. no more monthly humiliation.
Angela Spagnolo December 27, 2025
I just... I just wish people understood that a negative test doesn’t mean you’re lying. It means the test is broken. I take my meds. Every. Single. Day. But the screen doesn’t catch them. And then I get looked at like I’m some kind of criminal. It’s not fair. It’s not right. It’s just... sad.
SHAKTI BHARDWAJ December 28, 2025
Oh please. This whole system is just a way for Big Pharma and labs to make money. Urine tests don’t prevent overdoses-they just make patients feel like suspects. If you really cared about safety, you’d fund better treatment, not more tests. This is capitalism disguised as medicine.
Zina Constantin December 28, 2025
As someone who works in global health, I’ve seen how this plays out in low-resource settings. In places without LC-MS machines, patients are either misdiagnosed or denied care. We need affordable, accurate tech-not just in the U.S., but everywhere. This isn’t just a medical issue. It’s a human rights issue.
wendy parrales fong December 29, 2025
my cousin was on oxycodone for years. one time she tested negative and they almost cut her off. turns out the test didn’t even look for oxycodone. she cried for hours. no one should have to prove they’re not a drug addict just to get pain relief.
Jody Kennedy December 29, 2025
you guys need to stop treating patients like criminals. we’re not trying to hide anything-we’re trying to survive. if your test can’t detect the drug you prescribed, that’s YOUR problem, not mine. fix the system, not the person.
Dan Alatepe December 30, 2025
bro... i once took a test and it came back clean for everything except... i had a bag of poppy seed muffin for breakfast. they thought i was on heroin. 😅 they made me do a second test. i swear, this system is wild.
Sarah Holmes December 30, 2025
It is profoundly disturbing that we have allowed the medical establishment to reduce human suffering to a binary algorithm: positive or negative. The soul of medicine is not in the laboratory report-it is in the quiet, unspoken understanding between healer and healed. When we prioritize data over dignity, we do not heal-we surveil. And surveillance, no matter how well-intentioned, is never care.
Jay Ara December 31, 2025
good point about risk stratification. my doc uses the ORT and it made me feel like a person not a case file. also-pls ask your lab if they test for hydrocodone. most dont. i learned the hard way.
Matthew Ingersoll January 1, 2026
One of the most important things this post got right: testing isn’t about punishment. It’s about prevention. The fact that some clinics still use outdated panels is unacceptable. We need to demand better-not just for patients, but for doctors too. This isn’t just medical-it’s moral.