Imagine waking up and realizing that your body has suddenly stopped producing a hormone it needs to survive. For someone with Type 1 Diabetes is a chronic autoimmune condition where the immune system attacks and destroys insulin-producing beta cells in the pancreas, this is the reality. Unlike type 2 diabetes, which often develops slowly over years due to lifestyle and genetics, type 1 usually hits fast and hard. It isn't about eating too much sugar; it's an internal glitch where the body essentially locks its own doors, preventing glucose from entering cells for energy.
Dealing with this condition is a full-time job. According to the University of Michigan Health, it affects about 5-10% of all diabetes cases. While it can feel overwhelming at first, modern medicine has turned a once-fatal diagnosis into a manageable lifestyle. The goal is simple but demanding: keep blood sugar levels steady to avoid short-term crises and long-term damage to the heart, kidneys, and eyes.
The Red Flags: Spotting the Symptoms
Type 1 diabetes doesn't usually whisper; it screams. Because the body can't move sugar into the cells, the glucose builds up in the bloodstream, and the body goes into a state of starvation despite eating. This leads to a few classic signs that often appear over a few days or weeks.
- Extreme Thirst and Frequent Urination: When blood sugar spikes, the kidneys work overtime to filter it out, pulling water from your tissues. This leaves you feeling parched and running to the bathroom constantly.
- Unexplained Weight Loss: Since your cells can't access glucose for fuel, your body starts burning fat and muscle for energy. You might be eating more than usual but still losing weight.
- Crashing Fatigue: Without sugar getting into your cells, you're essentially running on an empty tank, leading to a level of exhaustion that sleep doesn't fix.
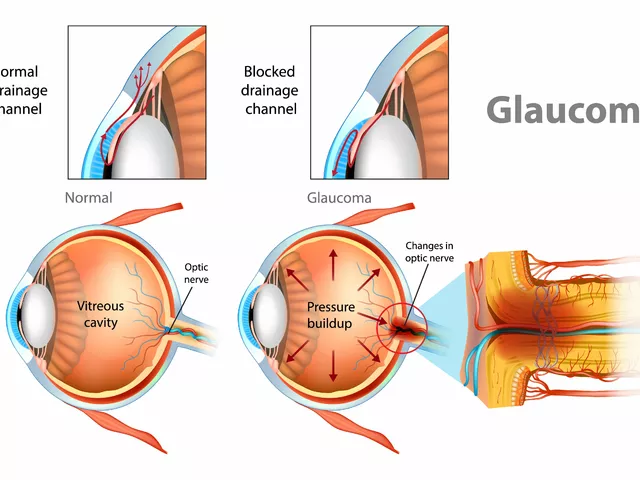
- Blurred Vision: High glucose levels can cause the lenses in your eyes to swell, making things look fuzzy.
In some cases, symptoms escalate rapidly into Diabetic Ketoacidosis (DKA), a life-threatening emergency. If you notice a fruity smell on the breath, nausea, or confusion, it's a sign that the blood has become acidic due to a buildup of ketones. This can happen within 24 hours if left untreated, making early recognition critical.
Getting a Clear Answer: The Diagnosis Process
If you suspect something is wrong, doctors won't rely on just one test. They use a combination of blood sugar snapshots and long-term averages to confirm the diagnosis and differentiate it from type 2.
The A1C Test is the gold standard for looking at the big picture. It measures your average blood sugar over the past three months. A result of 6.5% or higher on two separate tests usually confirms diabetes. However, for a quick look, a fasting plasma glucose (FPG) test of 126 mg/dL or higher after an 8-hour fast is a major indicator.
| Test Type | Diabetes Threshold | What it Measures |
|---|---|---|
| A1C Test | ≥ 6.5% | 3-month glucose average |
| Fasting Plasma Glucose | ≥ 126 mg/dL | Blood sugar after 8+ hours fasting |
| Random Plasma Glucose | ≥ 200 mg/dL | Blood sugar at any time (with symptoms) |
| Oral Glucose Tolerance | ≥ 200 mg/dL | Blood sugar 2 hours after glucose drink |
To prove it's specifically Type 1, doctors look for autoantibodies. Since this is an autoimmune disease, your blood will contain markers like GAD65 or IA2 antibodies. They also check C-peptide levels. C-peptide is a byproduct of insulin production; in Type 1, these levels are typically very low because the pancreas has stopped making insulin, whereas in Type 2, they are often high.
Insulin Therapy: Choosing Your Path
Since the body can no longer make its own insulin, you have to provide it manually. There are two main ways to do this, and the choice often depends on your lifestyle and how much control you want over the process.
Multiple Daily Injections (MDI)
This is the traditional "basal-bolus" method. You take a long-acting insulin once or twice a day to keep a steady baseline (basal) and then take rapid-acting insulin right before meals (bolus) to handle the glucose spike from food. It's a flexible approach, but it requires a lot of finger-pricking to monitor sugars and precise carbohydrate counting.
Insulin Pumps and Automated Systems
A Continuous Subcutaneous Insulin Infusion (CSII) system, or insulin pump, is a small device worn on the body. Instead of several needles a day, a catheter delivers insulin continuously. The real game-changer here is the integration with Continuous Glucose Monitoring (CGM). Modern "hybrid closed-loop" systems, like the Medtronic MiniMed 780G, act like an external pancreas. They read your sugar levels in real-time and automatically adjust insulin delivery, significantly increasing your "time-in-range" (the percentage of the day your sugar stays between 70-180 mg/dL).
The Daily Grind: Practical Management
Managing Type 1 is a mental and physical marathon. Patients often spend 2 to 4 hours every day just thinking about and treating their condition. It's not just about the shots; it's about the math. You have to calculate your insulin-to-carbohydrate ratio-for example, some people need 1 unit of insulin for every 10 grams of carbs, while others might need 1 unit for 15.
One of the scariest parts of this journey is hypoglycemia, or "lows." When blood sugar drops below 70 mg/dL, you might feel shaky, sweaty, or confused. The rule of thumb is the "15-15 rule": eat 15 grams of fast-acting carbs (like 4 oz of juice) and wait 15 minutes to re-check. If you're still low, repeat the process.
Beyond glucose, you have to keep an eye on other health markers. Because diabetes affects the whole body, regular check-ups for kidney function, liver health, and thyroid levels are mandatory. The American Diabetes Association generally suggests getting an A1C test every three to six months to ensure the treatment plan is actually working.
New Frontiers and Future Hope
The landscape of T1D is changing fast. For the first time, we have disease-modifying therapies. A drug called Teplizumab (Tzield) can actually delay the onset of clinical Type 1 diabetes in high-risk individuals. In clinical trials, this monoclonal antibody delayed the need for insulin for an average of 24.5 months, giving people more time to prepare.
Looking even further ahead, researchers are working on stem-cell therapies. Vertex Pharmaceuticals has seen success with the VX-880 trial, where stem-cell-derived islet cells were infused into patients. Some participants actually achieved insulin independence, meaning their new cells started doing the job the original pancreas couldn't. While not yet available to the general public, it's a glimpse into a future where "management" becomes a "cure."
Can Type 1 Diabetes be cured with diet?
No. Type 1 diabetes is an autoimmune condition where the pancreas stops producing insulin. While a healthy diet helps manage blood sugar levels and reduces complications, it cannot restart insulin production. Lifelong insulin therapy is required for survival.
What is a target A1C for someone with T1D?
For most adults, the general target is an A1C of less than 7%. However, this is individualized. Depending on your age, other health issues, or how often you experience severe lows, your doctor might set a target between 6.5% and 8.0%.
How often should I check my blood sugar?
If you use traditional finger-stick monitors, you may need to check 4 to 10 times a day, including before meals and before bed. If you use a Continuous Glucose Monitor (CGM), you get real-time readings every few minutes, which provides a much more complete picture of your glucose trends.
What is the difference between Type 1 and Type 2?
Type 1 is an autoimmune attack that destroys insulin-producing cells, often appearing suddenly in childhood or young adulthood. Type 2 is a condition where the body becomes resistant to insulin or doesn't make enough, usually developing slowly over time and often linked to genetics and lifestyle.
Is a CGM better than a finger-stick meter?
For most, yes. CGMs provide a continuous stream of data and alerts for highs and lows, which studies show can reduce A1C by 0.4% to 0.8%. However, some people still use finger-sticks to calibrate their sensors or as a backup when the sensor readings feel inaccurate.





Doug DeMarco April 12, 2026
CGMs are seriously a life saver for anyone just starting out! :) It's so much better than stabbing your finger ten times a day and guessing what's happening inside. If anyone is struggling with the cost, definitely look into patient assistance programs because you shouldn't have to go without this tech!
Rakesh Tiwari April 14, 2026
Oh wow, a guide that tells us we need insulin to survive Type 1. Truly revolutionary stuff here. I'm sure the medical establishment is shaking in their boots now that we've discovered that autoimmune diseases actually require medicine.
emmanuel okafor April 15, 2026
it is strange how the body just decides to fight itself one day and everything changes forever
Camille Sebello April 16, 2026
Wait... how old were you when you got diagnosed??? Do you actually use a pump??? I need to know the brand!!!
Simon Jenkins April 16, 2026
The utter audacity of some people to think MDI is a viable 'choice' in the modern era is simply staggering. I mean, really! Why would anyone voluntarily subject themselves to the primitive torture of multiple daily injections when closed-loop systems exist? It's practically medieval! The sheer psychological toll of manual carb counting is a nightmare that most of you simply cannot comprehend unless you've lived through the absolute tragedy of a 300 mg/dL spike while trying to enjoy a simple piece of cake. It's an absolute catastrophe of human existence!
Sarina Montano April 17, 2026
The mention of Teplizumab is such a glimmer of hope. It's a fascinating mechanism of action, essentially acting as a molecular shield to preserve those precious beta cells before they're completely decimated. For those who aren't familiar, this kind of immunotherapy is a complete paradigm shift from just treating the symptoms to actually altering the disease trajectory. It’s like catching a fire before it burns down the whole house instead of just trying to put out the embers.
Franklin Anthony April 18, 2026
interesting how they push these new drugs like tzield’s and stem cells’ now. makes you wonder who really profits when we just delay the inevitable instead of looking at what’s actually triggering these autoimmune spikes in the first place. stay safe everyone
Victor Parker April 19, 2026
Exactly!! 🙄 Big Pharma just wants us on these pumps forever so they can collect subscription fees for the sensors. Wake up people! They don't want a cure, they want a customer! 💉💰
Emily Wheeler April 20, 2026
I truly feel that the journey of living with T1D is less about the numbers on a screen and more about the resilience of the human spirit in the face of a constant, invisible battle, and while the math can be daunting, I believe that by supporting each other and sharing our collective wisdom, we can all find a way to coexist with this condition in a way that empowers us rather than defines us, because ultimately we are all just trying to find balance in a world that feels incredibly unbalanced sometimes.
Peter Meyerssen April 20, 2026
The homeostasis is basically a socio-biological construct 🙄. The glycemic variability is just a manifestation of the entropy of the pancreas. It's quite simple if you understand the metabolic pathways. 💅
Ryan Hogg April 20, 2026
I remember my first DKA episode and the terror of not knowing why I was shaking. It's a void that never really goes away, just a constant humming anxiety in the back of my mind that I'm one missed bolus away from a crisis. Every time I see a needle, I'm reminded of the hospital smells and the feeling of total helplessness. It's just exhausting to keep fighting a war against your own organs every single second of every single day.